Research Article
Features of Interferon and Cytokine Status in Atopic Dermatitis

Ospelnikova TP*, Gevorkyan OV, Mironova TV, Andreeva SA, Kolodyazhnaya LV and Ershov FI
Federal State Budgetary Institution, “Federal Research Centre of Epidemiology and Microbiology named after the Honorary Academician N.F.Gamaleya” of the Ministry of Health of the Russian Federation, Gamaleya Street, 18, Moscow, Russian Federation, 123098
*Address for Correspondence: Tatiana Ospelnikova, Federal State Budgetary Institution, “Federal Research Centre of Epidemiology and Microbiology named after the Honorary Academician N.F.Gamaleya” of the Ministry of Health of the Russian Federation, Russian Federation, Email: [email protected]
Dates: Submitted: 20 April 2017; Approved: 26 May 2017; Published: 29 May 2017
How to cite this article: Ospelnikova TP, Gevorkyan OV, Mironova TV, Andreeva SA, Kolodyazhnaya LV, et al. Features of Interferon and Cytokine Status in Atopic Dermatitis. Arch Asthma Allergy Immunol. 2017; 1: 009-014. DOI: 10.29328/journal.aaai.1001002
Copyright License: © 2017 Ospelnikova TP, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Atopic dermatits; Cytokines; Herpes virus; Interferon inducer Cycloferon; ELISA

ABSTRACT
The insufficiency of interferon production and the cytokine imbalance in patients with atopic dermatitis, especially in combination with persistent herpes virus infection, has been identified. The expediency of the use of interferon inducer Cycloferon in the treatment of chronic atopic dermatitis has been shown.
INTRODUCTION
Atopic dermatitis (AD) is one of the most common chronic relapsing inflammatory skin and allergic diseases [1-3]. AD refers to socially significant diseases. This disease retains its clinical signs for many years, it is often transformed into bronchial asthma with a severe atopic syndrome or into a systemic disease damaging not only the skin, but also internal organs such as digestive, respiratory, urinary systems [4,5]. The search for effective preventive and curative drugs aimed to improve the quality of life of patients with AD is one of the important problems for allergists, immunologists, dermatologists [6].
It is known that immunological imbalance, along with a genetic predisposition, plays almost the main role in the AD pathogenesis. It has been established that the leading immunopathological mechanism in the development of AD is a change in the ratio of Th1/Th2-lymphocytes in favor of the latter with the appearance of characteristic IgE reactivity and high production of specific IgE antibodies to various exoallergens. At the same time, there are data on the involvement of cell-mediated, allergic reactions in the immunopathogenesis of AD, especially in its chronic severe forms [7].
AD is characterized by impairments in the system of innate immunity and barrier properties of the skin, which explains the increased sensitivity of AD patients to various infectious diseases. Activated CD4+cells with the Th2 phenotype dominate in the damaged areas of AD patient’s skin, which contribute to the enhancement of IgE production by B lymphocytes. The overwhelming number of patients showed positive responses of immediate type in skin testing with inhalation (home dust mites and animal dander) or food allergens [8]. It was also revealed that in the CD3-positive cells of the peripheral blood of patients with AD, the expression of the ETEA gene was sharply increased, the product of which (a protein of 445 amino acids) plays a role in regulating the sensitivity of T cells and eosinophils to proapoptotic stimuli [9].
Along with atopy, autoimmune reactions that determine the chronic recurrent course of the disease may play a role in the mechanism of AD formation. Perhaps the involvement of autoreactivity in the pathogenesis of AD, in particular, the immune response to human proteins located in cells of different organs, such as the skin, lungs, muscles and brain. Moreover, exacerbation of AD in certain patients has been associated with an increase in IgE-autoreactivity [10].
Insufficient production of interferons (IFN) as the most important factors of innate immunity, plays an important role in the pathogenesis of AD, aggravating the course of the disease, increasing the duration of exacerbation, and reducing remissions.
The purpose of this work was to study the features of immunological reactivity disorders by determining the IFN and cytokine status in patients with AD and the effectiveness of their correction by Cycloferon - the domestic low-molecular IFN inducer.
MATERIALS AND METHODS
Material for the study. Blood (heparinized and blood serum) from 14 practically healthy people (control group) and from 15 patients with AD (in the acute stage).
Patients
A set of patients with AD was selected on the basis of Moscow City Clinical Hospital No. 14 named after. V.G. Korolenko. There were 15 patients with AD under observation, aged from18 to 25 years (9 women and 6 men); all patients were in an aggravation stage. The diagnosis of AD was based on clinical and laboratory data. The study protocol was approved by the local ethic committees Moscow City Clinical Hospital. All the patients signed written informed consent and donated samples of blood. Patients have clinical manifestations from early childhood. The degree of severity of the disease was determined during the period of exacerbation, at the time of admission to the clinic. 8 patients with AD had moderate severe course of the disease (frequency of exacerbations 3-4 times a year, duration of remission 2-3 months), in 7 patients there was a severe course (frequency of exacerbations 5 times a year, short period of remission of 1-2 months). In all patients, the process was widespread (lesion area 46-49%), represented by erythematous-squamous foci with excoriation and white dermographism. In 85% of patients in case history there were clinical manifestations of herpetic infection (Herpes simplex), at the time of the examination the herpetic eruptions were not manifested. Eosinophilia was detected in 95% of patients in a clinical blood test. Worms’s invasions are excluded in all examined patients. The level of IgE was increased in 70% of the subjects. As a control group, 14 practically healthy men and women were examined, aged from 25 to 55 years, who had no history of allergic manifestations and there was no hereditary complication.
All groups were assessed with IFN and cytokine status, in patients with AD at admission and after treatment. Clinical observations were conducted within a year. Patients received basal therapy (antihistamines, detoxification, hyposensitizing drugs), after treatment of acute exacerbations, Cycloferon was added 2.0 ml intramuscularly in the scheme: 1, 2, 4, 6, 8, 11, 14, 17, 20, 23 days of injection.
Cycloferon
Meglumine acridоnacetate is a domestic low-molecular inducer of IFN (“Polisan”, Russia). Previously, it was shown that the drug is an inducer of interferons and other cytokines activating the cellular and humoral immune response (Th1/Th2). In addition, it enhances the functional activity of neutrophilic granulocytes, activates phagocytosis, increases the generation of reactive oxygen species by phagocytic cells. The anti-inflammatory effect of Cycloferon is due to a dose-dependent inhibitory effect on the synthesis of proinflammatory cytokines (IL-1b, IL-8 and TNF-a), as well as mononuclear production of anti-inflammatory cytokines IL-10 and/or TGF-b.
METHODS
IFN status including circulating IFN; level of IFNα production by leukocytes infected with Newcastle disease virus; level of IFNγ production by lymphocytes induced by 10 µg/ml FGA («Difco»), level of spontaneous IFN production in vitro were assayed in whole heparinized blood. Units/ml of IFN were calculated as reverse dilutions protecting 50% of cellular monolayers from the virus-induced cytopathic effect [11].
ELISA
For the cultivation and mitogen stimulation of blood cells, a set of kit-reagents “Cytokin-Stimul-Best” was used and the concentration of IFN-α, IFN-γ, IL-1b, IL-6, IL-8, IL-17, IL-2, IL-4, IL-10, TNF-α was determined using the ELISA kits «Vector-Best» (Russia) and IL-13 (“Bender MedSystems”, Austria).
Statistical processing of the data was carried out using the BIOSTAT program (calculation of M±σ, reliability of differences in the mean values from the paired Student test).
RESULTS
It was found that the majority of patients with exacerbation of AD in clinical analysis of the blood showed eosinophilia (95%) and increased concentration of IgE (70%) in the blood serum. All patients had a recurring course of the disease in the phase of exacerbation (3-5 exacerbations per year). The study of the IFN system by a biological method revealed differences in the rates between the examined and control groups. As can be seen from figure 1, in all the examined patients with AD, the IFN system was deficient in the production of α- and, especially, γ-IFN with blood leukocytes. The average IFN status was (in U/ml): the ability to produce α-IFN blood leukocytes 174.7±17.94; IFN-γ-12.53±0.77; serum IFN-7.87±2.32; spontaneous IFN-0.2±0.11. The titer of serum IFN was elevated in 6 patients (40%); the presence of spontaneous IFN-in 3 patients (20%).
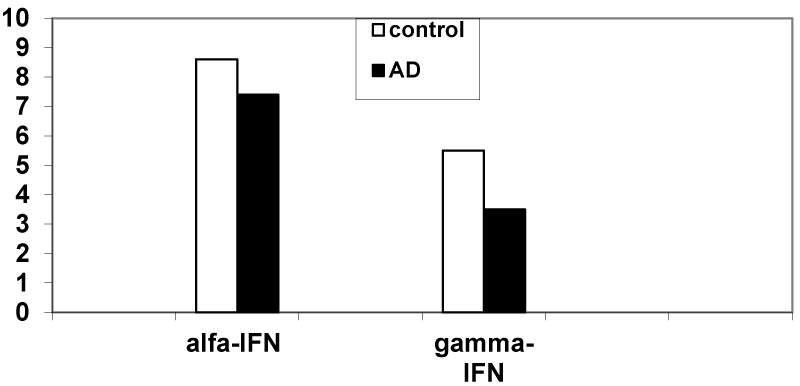
Figure 1: Production of IFN-α and IFN-γ (U/ml) by blood leukocytes in patients with AD (p<0.05) (log2 scale).
Analyzing the data obtained to determine the levels of cytokines in the blood, we can note a number of features in patients with AD compared with healthy donors (control group). An increased content of proinflammatory cytokines, especially IL-8 (p<0.05), to a lesser extent, IL-6 (p>0.05), and at the same time a significant decrease in IL-2 (p<0.05) (Figure 2). Of the 15 patients, 5 values of serum IL-8 exceeded 100 pg/ml (97 to 575 pg/ml). After the treatment, the normalization of these indicators was noted. Serum TNF-α was detected in 3 (20%), IL-1β - in 5 patients out of 15 (33.3%).
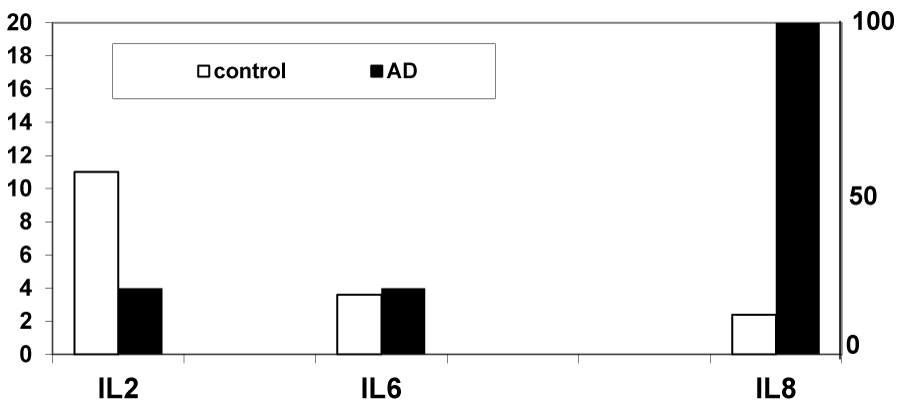
Figure 2: The content of cytokines (pg/ml) in the serum of blood in patients with AD.
It is known that Th2 cells are responsible for the development of the immune response of the humoral type and the hyperproduction of IL-4, IL-10, IL-13 in allergic diseases. However, IL-4 was not detected in the serum of the patients with AD, IL-10 was detected in 1 patient (6.7%), IL-13 in 3 patients (20%).
It should be noted that IFN-α and IFN-γ were not detected in the serum of patients with AD, although induced and spontaneous production of both types of IFN was observed, which was 4.5 times and 1.5 times (respectively) less pronounced in patients with AD, than in the samples of the control group (Figure 3). Between spontaneous and induced interferons production there is a statistically significant difference (p<0.05).
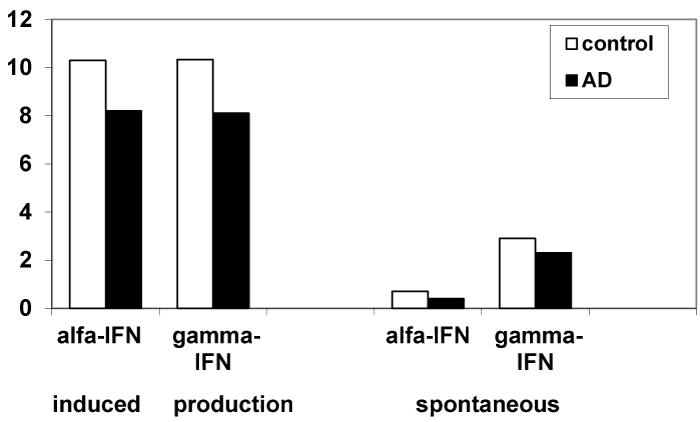
Figure 3: Induced and spontaneous production of IFN-α and IFN-γ (pg/ml) by blood leukocytes in patients with AD (log2 scale).
As can be seen from figure 4, significant (p<0.05) positive dynamics of interferon production with blood leukocytes with a tendency toward normalization, as well as normalization of serum IFN levels and the disappearance of spontaneous IFN in the in vitro reaction was noted after treatment with Cycloferon. In addition, the levels of proinflammatory cytokines, such as IL-8 and IL-6, in the blood serum after treatment, with a parallel increase in IL-2 and IFN-a, should be noted.
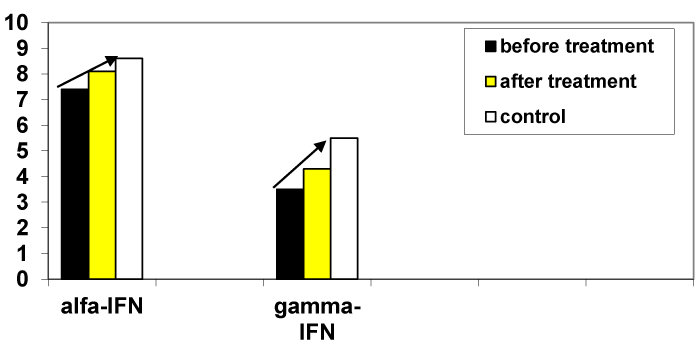
Figure 4: Production of IFN-α and IFN-γ (U/ml) by blood leukocytes in patients before and after treatment (log2 scale).
The combination of immune system disorders with the lack of ability to produce α- and γ-IFN by blood leukocytes in patients with revealed responsiveness of blood leukocytes to the IFN inducer Cycloferon gives grounds to consider it appropriate to use it in therapy of patients with AD exacerbations immediately after the basic therapy.
After complex therapy, there was a positive clinical dynamics in the form of: reducing erythema, reducing the intensity of itching, stopping the appearance of new elements, preservation of lichenification, as well as reducing the number of exacerbations and increasing the duration of remission.
DISCUSSION
As follows from the data obtained, with AD develops a pronounced IFN deficiency, especially the production of γ-IFN of blood leukocytes. There arises a completely natural assumption: are the defects of innate immunity one of the causes of AD? It is known that a prolonged persistence of viruses leads to secondary immunodeficiency, while in turn secondary immunodeficiency promotes the activation of the viruses themselves [12,13]. In any case, in the pathogenesis of the disease, the immune competence of the patient’s body is of great importance. Against the background of IFN-immune deficiency may often occur exacerbations of AD.
In this connection, the inclusion of IFN inducers in therapy seems reasonable. Its immune regulatory properties are mediated through the activation of IFN-γ. An increase in its production contributes to the restoration of the T-cell link of immunity: it normalizes the levels of subpopulations of CD3+, CD4+, CD8+, as well as the number of CD16+, CD72+. Earlier it was shown that the use of Cycloferon is quite effective in patients with chronic and recurrent viral and bacterial infections and in patients with a secondary immunodeficient status (herpetic and cytomegalovirus infections) [13]. Cycloferon therapy is also relevant for patients with relapsing AD. The treatment with Cycloferon reduced the number of exacerbations and increased the duration of remission in patients with AD.
The ability of blood leukocytes to produce cytokines under the influence of stimuli is clearly pronounced, and the ability of leukocytes of patients with AD to IFN-γ synthesis is significantly higher than the synthesis of IL-4, i.e. there is clearly a classical picture of the production of cytokines in the long-term inflammatory process. In our case, this is a chronic relapsing form of AD, which is very difficult to treat. The vast majority (85%) of the examined patients with AD have a persistent herpesvirus infection, which, as is known, can lead the patient’s body to the state of IFN-immune deficiency. It is known that these viruses affect more than 1/3 of the population worldwide and are responsible for a wide range of human diseases, ranging from mild herpesvirus infection to disseminated forms such as Eczema herpeticatum in patients with atopic eczema or in those with severe immunodeficiency. These viruses have an intracellular location, displaying a clinically latent persistent form of the disease. In addition, viruses of the Herpesviridae are able to influence the normal functioning of regulatory cells of the Treg, weighting the course of the underlying disease.
IL6, IL8 and IFN-γ serve as mediators of subacute and chronic inflammation in atopic dermatitis. The decrease in the level of proinflammatory cytokines, especially IL8, after complex treatment, as well as an increase in IL2 level, indicates a decrease in the inflammatory process.
The absence of IFN-a in the serum can lead to recurrent infections [14]. IFN-γ, secreted by activated viral antigen Th1 lymphocytes, can suppress the reproduction of the virus, disrupting the intracellular processes of viral replication. However, this mechanism does not work well or does not work at all if there is a deficiency/defect in the IFN system (for example, in herpetic infection). Induced (by various stimuls, mitogens) synthesis of cytokines reflects the potential, reserve capacity of cells to respond to an antigenic stimulus (in particular, the action of drugs). Reduced induced production of cytokines in vitro can serve as one of the signs of an immunodeficiency state.
With the action of various viral agents and Cycloferon, a whole cascade of signals is induced, which involve the “cytokine network” of the organism. As is known, the functioning of the immune system is built on the balance of lymphocytes (Th1 and Th2) and on equivalent production of the appropriate regulatory cytokines [15]. One of the important directions in the formation of a full-fledged immune response is the regulation of the synthesis of IFNs. The production of IFN-γ Th1 by cells and NC is carried out by stimulation with so-called IFN-γ-inducing cytokines, such as IL-12, IL-2 and TNF-a. In addition, IL-18, being a potential inducer of IFN-γ synthesis, acts as a synergist of IL-12, and both these cytokines lead in the rapid activation of the monocyte / macrophage system by stimulating the production of IFN-γ, which is actively stimulated by the action of Cycloferon.
Thus, the new knowledge about the imbalance of cytokines in AD makes it possible to add an additional criterion for the severity of this uneasy allergic disease (decreased ability to produce IFN-a and especially IFN-γ by blood leukocytes by a biological method, an increased level of IL-8 and IL-6 in serum, especially significant in patients with burden of the disease, a reduced level of IL-2) for further exposure to therapeutic agents.
REFERENCES
- Corren J. Inflammatory Disorders Associated with Allergy: Overview of Immunopathogenesis and Implications for Treatment. Immunol Allergy Clin North Am. 2017; 37: 233-246. Ref.: https://goo.gl/sJp55z
- Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014; 71: 116-132. Ref.: https://goo.gl/VKCCdO
- Ong PY, Leung DY. Atopic dermatitis. Clin Allergy Immunol. 2002; 16: 355-379. Ref.: https://goo.gl/CSE6rP
- Ohshima Y, Yamada A, Hiraoka M, Katamura K, Ito S, et al. Early sensitization to house dust mite is a major risk factor for subsequent development of bronchial asthma in Japanese infants with atopic dermstitis: results of a 4-year followup study. Ann Allergy Asthma Immunol. 2002; 89: 265-270. Ref.: https://goo.gl/Dt9mSx
- Krakowski AC, Eichenfield LF, Dohil MA. Management of atopic dermatitis in the pediatric population. Pediatrics. 2008; 122: 812-824. Ref.: https://goo.gl/UvI7RF
- Hanifin JM, Cooper KD, Ho VC, Sewon K, Bernice RK, et al. Guidelines of care for atopic dermstitis. J Am Acad Dermatol. 2004; 50: 391-404. Ref.: https://goo.gl/eLCGe4
- Maintz L, Novak N. Modifications of the innate immune system in atopic dermatitis. J Innate Immun. 2011; 3: 131-141. Ref.: https://goo.gl/fjIPwn
- Zeiger RS, Heller S, Mellon MH, Forsythe AB, O'Connor RD, et al. Effect of combined maternal and infant food-allergen avidance on development of atopy in early infancy: a randomized study. J Allergy Clin Immunol. 1989; 84: 72-89. Ref.: https://goo.gl/PE8xyl
- Imai Y, Nakada A, Hashida R, Sugita Y, Tanaka T, et al. Cloning and characterization of the highly expressed ETEA gene from blood cells of atopic dermatitis patients. Biochem and Biophys Res Commun. 2002; 297: 1282-1290. Ref.: https://goo.gl/4WYYE5
- Valenta R, Kraft D. From allergen structure to new forms of allergen-specific immunotherapy. Current Opin Immunol. 2002; 14: 718-727. Ref.: https://goo.gl/P8qy4K
- Ospelnikova TP, Konisheva AV, Mazurina SA, Lyzogub NV, Osipova VV. Evaluation of interferon system and the main cytokines in patients with bronchial asthma. J Microbiol, Epidemiol, Immunol. 2012; 1: 35-41. Ref.: https://goo.gl/DnkLld
- Ong PY, Leung DY. Bacterial and Viral Infections in Atopic Dermatitis: a Comprehensive Review. Clin Rev Allergy Immunol. 2016; 51: 329-337. Ref.: https://goo.gl/YCC5Cz
- Ershov FI, Ospelnikova TP Modern arsenal of antiherpetic drugs. Infections and Antimicrobial Therapy. 2001; 4: 100-104.
- Simbirtsev AS. Cytokines: classification and biological functions. Cytokines and inflammation. 2004; 2: 16-23. Ref.: https://goo.gl/s08PNm
- O’Shea JJ, Averil М, Lipsky Р. Cytokines and autoimmunity. Naturе Reviews Immunology. 2002; 2: 37-45. Ref.: https://goo.gl/Qncl40